

Abstract
Menopausal transition is highly symptomatic in at least 20% of women. A higher prevalence of psychiatric symptoms, including depression, anxiety, and sleep disturbance, has been shown in women with symptomatic menopausal transition. However, a clear correlation between symptomatic menopausal transition and psychiatric disorders has not been established.
We explored the association between symptomatic menopausal transition and subsequent newly diagnosed psychiatric disorders, including schizophrenia as well as bipolar, depressive, anxiety, and sleep disorders.
We investigated women who were diagnosed with symptomatic menopausal transition by an obstetrician-gynecologist according to the data in the Taiwan National Health Insurance Research Database. A comparison cohort comprised age-matched women without symptomatic menopausal transition. The incidence rate and the hazard ratios of subsequent newly diagnosed psychiatric disorders were evaluated in both cohorts, based on the diagnoses of psychiatrists.
The symptomatic menopausal transition and control cohorts each consisted of 19,028 women. The incidences of bipolar disorders (hazard ratio [HR] = 1.69, 95% confidence interval [CI] = 1.01–2.80), depressive disorders (HR = 2.17, 95% CI = 1.93–2.45), anxiety disorders (HR = 2.11, 95% CI = 1.84–2.41), and sleep disorders (HR = 2.01, 95% CI = 1.73–2.34) were higher among the symptomatic menopausal transition women than in the comparison cohort. After stratifying for follow-up duration, the incidence of newly diagnosed bipolar disorders, depressive disorders, anxiety disorders, and sleep disorders following a diagnosis of symptomatic menopausal transition remained significantly increased in the longer follow-up groups (1–5 and ≥ 5 years).
Symptomatic menopausal transition might increase the risk of subsequent newly onset bipolar disorders, depressive disorders, anxiety disorders, and sleep disorders. A prospective study is necessary to confirm these findings.
INTRODUCTION
Menopausal transition is a period late in a woman's reproductive life before the final menstrual period. Menopause is a physiological phase defined retrospectively by 12 months of amenorrhea and loss of ovarian follicular function, typically occurring in most women between the ages of 40 and 55 years. The mean duration of menopausal transition is 5 years, but symptoms during this period may begin 8 years or more before the final menstrual period.1
Although the menopausal transition is not a disease and does not require diagnosis or treatment unless symptoms are present, for clinicians, early awareness of symptoms of menopausal transition is essential for providing appropriate counseling or treatment. In general, symptomatic menopausal transition is a clinical diagnosis. Accordingly, laboratory testing, including determining follicle-stimulating hormone and estradiol levels, is not necessary for establishing the diagnosis, and skilled clinicians can diagnose symptomatic menopausal transition based on the characteristic symptoms such as abnormal uterine bleeding, hot flashes, and night sweats, which occur as a result of declining ovarian function.2 It is clear that the existence and severity of symptoms during the menopausal transition are strongly related to the woman's quality of life.3
Regardless of ethnic origin, skin color, or socio-demographic factors, women around the world suffer not only from characteristic somatic symptoms of the menopausal period,4 such as hot flushes, night sweats, lowered metabolism, and sexual problems, but also from psychiatric symptoms, such as changes in mood, anxiety, and sleep disturbance.5 However, in clinical practice, the diagnosis of symptomatic menopausal transition is based more on the somatic rather than psychiatric symptoms.6,7 Nevertheless, experts in symptomatic menstrual transition recognize that psychiatric problems are a core issue among affected women. However, most studies focusing on the evaluation of occurrence or severity of psychiatric symptoms during menstrual transition employ rating scales or other self-reporting methods8–13 rather than clinical diagnostic interviews to identify psychiatric disorders. Oftentimes, the self-reported depression, anxiety, and sleep disturbance can be tolerated by the patients or treated by their primary care physicians or obstetrician-gynecologists. Accordingly, the knowledge on the incidence of clinical depression, anxiety, and sleep disorders in women with symptomatic menopausal transition is currently very limited.
Several studies dedicated to menopausal transition in women with schizophrenia14,15 and bipolar disorder16–18 investigated changes in psychotic symptoms and mood course fluctuations. In addition, about 3 decades ago, Kukopulos et al19 and Oppenheim20 provided evidence that treatment of unipolar depression during menstrual transition with antidepressants or augmentation with estrogen may increase the risk of a bipolar switch, especially in those with features of rapid cycling. However, nationwide clinical data regarding the association between menopausal transition and risk of developing subsequent newly diagnosed schizophrenia and bipolar disorders (especially in those without past history of depression) are limited.
In this study, we focused on psychiatric symptoms severe enough to require evaluation by a specialist and warrant a diagnosis of a psychiatric disorder. In particular, we designed a retrospective cohort study using a nationwide claims database to investigate the possible link between symptomatic menopausal transition and psychiatric disorders.
PATIENTS AND METHODS
Data Sources
The National Health Insurance (NHI) program has been implemented in Taiwan since 1995, offering comprehensive and universal medical care coverage to all citizens, with a coverage rate of up to 98%.21 In the present study, the data were analyzed from the Longitudinal Health Insurance Database 2000 (LHID 2000), which is a subset of the NHI Research Database (NHIRD) and contains all original claims data for 1,000,000 random subjects in the Registry of Beneficiaries in 2000. The NHIRD contains information regarding clinical visits, including prescription details and diagnostic codes based on A-code and International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). A-code is a disease classification system developed specifically for filing medical claims that was mainly used for ambulatory care before 2000 in Taiwan. A-code is a much simplified version of ICD-9-CM. To maintain the consistence between different claim records and to reflect the true distribution of different diseases, the NHI program switched the disease coding to the ICD-9-CM codes in 2000. In our study, A-code was mainly used to exclude patients who were diagnosed with symptomatic menopausal transition between 1996 and 2000 as well as those diagnosed with psychiatric disorders before they were diagnosed with symptomatic menopausal transition. The NHIRD is released and managed by the National Health Research Institutes, and confidentiality is maintained according to the directives of the Bureau of NHI.
Ethics Statement
The Institutional Review Board of Kaohsiung Veterans General Hospital approved this study (VGHKS15-CT8-03). Written consent from the study subjects was not obtained because the NHI dataset consists of deidentified secondary data for research purposes, and the Institutional Review Board of Kaohsiung Veterans General Hospital issued a formal written waiver for consent for this study.
Study Population
Using data extracted from LHID 2000, we conducted a retrospective cohort study. In the study, we enrolled women who had newly diagnosed with symptomatic menopausal transition (ICD-9-CM code: 627.2) by an obstetrician-gynecologist between January 1, 2000, and December 31, 2008. The index date (the enrollment date) was defined as the date when an eligible woman with symptomatic menopausal transition was included in the cohort of symptomatic menopausal transition. For each woman included in the cohort of symptomatic menopausal transition, 1 age-matched woman without symptomatic menopausal transition served as a subject in the control cohort was randomly selected from LHID 2000. In both cohorts, women with a medical history of psychiatric disorders (A-codes: A210-A219; ICD-9-CM codes: 290–319) before the index date were excluded.
In the study, the major outcomes of interest are the psychiatrist-diagnosed psychiatric disorders, including schizophrenia (ICD-9-CM code 295), depressive disorder (ICD-9-CM codes 296.2, 296.3, 300.4, and 311), bipolar disorder (ICD-9-CM codes 296.0, 296.1, 296.4, 296.5, 296.6, 296.7, 296.8, 296.80, and 296.89), anxiety disorder (ICD-9-CM codes 300.0, 300.2, 300.3, 308.3, and 309.81), and sleep disorder (ICD-9-CM codes 780.5, 307.4 [excluding 780.51, 780.53, 780.57]). Therefore, each age-matched pair among both cohorts was observed from the index date until the occurrence of above-mentioned psychiatric disorders, or until death, withdrawal from the health insurance system, or December 31, 2013.
In psychiatry, there are only a few clearly defined and modifiable risk factors; therefore, most studies have focused on largely unmodifiable ones, such as age and sex, and the common physical comorbidities, such as hypertension, diabetes mellitus, dyslipidemia, coronary artery disease, congestive heart failure, chronic pulmonary disease, and malignancy as potential confounding factors. In our study, comorbidities were also defined based on ICD-9-CM codes, and variables such as age, comorbidities, urbanization, and monthly income were all determined on the index date in both cohorts.
Statistical Analysis
The incidences of newly diagnosed schizophrenia, bipolar disorders, depressive disorders, anxiety disorders, and sleep disorders in the symptomatic menopausal transition and control women were calculated, and independent t-tests and Chi-squared tests were conducted to examine the differences in the characteristics between the 2 cohorts. In addition, we calculated incidence rates (per 1000 person-years) and incidence rate ratios (IRRs) of these psychiatric comorbidities. Moreover, to investigate potential surveillance bias, subgroups were stratified according to the follow-up duration (0–1, 1–5, and ≥5 year) since symptomatic menopausal transition diagnosis. A follow-up of less than 1 year could introduce potential surveillance bias, which is frequently observed in claims database studies. In addition, although a recent epidemiologic study revealed that frequent vasomotor symptoms (VMS) generally lasted more than 7 years during the menopausal transition for more than half of women, race and ethnicity had a profound effect on total VMS duration, with a significantly shorter total VMS duration (around 5 years) observed in Chinese women.22 Therefore, a comparative analysis of cases with follow-up duration of 1–5 years and more than 5 years may reflect the influence of gradually disappearing VMS.
A Cox proportional hazard model was used for multivariate adjustment. Potential confounding factors such as age, comorbidities (as listed in Table 1), degree of urbanization, and monthly income were included in the univariate analysis separately. To better elucidate symptomatic menopausal transition as a dependent risk factor for subsequent psychiatric disorders, variables that demonstrated a moderately significant statistical relationship in the univariate analysis (P < 0.1) were put in a multivariate Cox proportional hazard regression model for multivariate adjustment (not shown in Table 1). In addition, the scaled Schoenfeld residuals test was performed to test the proportionality of hazards.
TABLE 1.
Characteristics of Women With Symptomatic Menopausal Transition and Control Subjects

The SAS statistical software for Windows, version 9.3 (SAS Institute, Cary, NC), was used for data extraction, computation, linkage, processing, and sampling. All other statistical analyses were performed using the SPSS statistical software for Windows, version 20 (IBM, Armonk, NY). A P value <0.05 was considered to indicate a statistically significant relationship.
RESULTS
Figure 1 displays the flowchart of enrollment. Our study sample comprised 19,028 symptomatic menopausal transition women and 19,028 control women. The basic characteristics of the 2 cohorts are shown in Table 1. The median age was 51.3 years (interquartile range, 46.4–56.9 years). Compared with the control cohort, the symptomatic menopausal transition cohort had higher percentages of comorbidities, significantly higher income, and higher degree of urbanization. During the entire follow-up period, 2164 (11.4%) symptomatic menopausal transition women and 1069 (5.6%) control women were diagnosed with psychiatric disorders (P < 0.001). The 3 most frequent types of psychiatric disorders detected in both cohorts were depressive disorders (4.6% vs 2.2%, P < 0.001), anxiety disorders (3.6% vs 1.7%, P < 0.001), and sleep disorders (2.8% vs 1.4%, P < 0.001).
FIGURE 1.
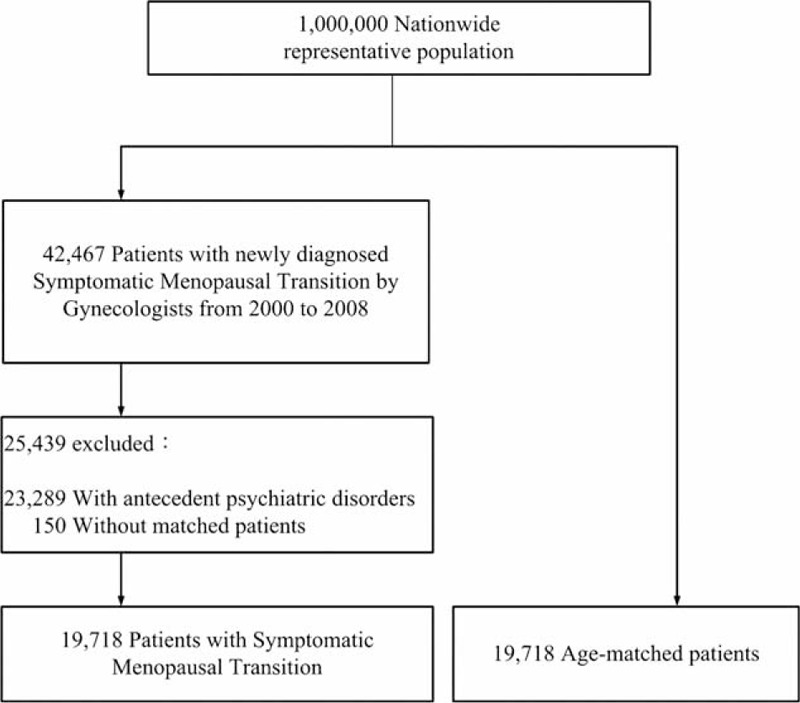
Flow diagram summarizing the process of enrollment.
As shown in Table 2, within the entire follow-up period, significantly higher IRRs of bipolar disorders (IRR = 1.71, 95% confidence interval [CI] = 1.01–2.96), depressive disorders (IRR = 2.15, 95% CI = 1.91–2.42), anxiety disorders (IRR = 2.07, 95% CI = 1.81–2.37), and sleep disorders (IRR = 2.01, 95% CI = 1.73–2.34) were observed in the symptomatic menopausal transition cohort than in the control cohort. Stratification according to follow-up durations revealed no significant differences in the incidence of schizophrenia in any group. However, IRRs of newly diagnosed depressive disorders, anxiety disorders, and sleep disorders remained significantly increased in all the follow-up duration groups (0–1, 1–5, and ≥5 year), and that of bipolar disorders increased only in the groups with a follow-up longer than 1 year (1–5 and ≥5 year).
TABLE 2.
Number of Newly Diagnosed Schizophrenia, Bipolar, Depressive, Anxiety, and Sleep Disorders Between Women With Symptomatic Menopausal Transition and Control Subjects Which Was Stratified by Follow-Up Duration

Table 3 compares crude hazard ratios (HRs) and adjusted hazard ratios (aHRs) of the newly diagnosed psychiatric disorders for the symptomatic menopausal transition women and controls. The crude HRs obtained with the univariate analysis revealed that patients with symptomatic menopausal transition may have an increased risk of developing a subsequent bipolar disorder, depressive disorder, anxiety disorder, and sleep disorder. The results of the multivariate analysis indicated that the women with symptomatic menopausal transition had a markedly higher risk of a subsequent depressive disorder (aHR = 2.17, 95% CI = 1.93–2.45), anxiety disorder (aHR = 2.11, 95% CI = 1.84–2.41), and sleep disorder (aHR = 2.01, 95% CI = 1.73–2.34). A small but significant increase in the risk of a subsequent bipolar disorder was also observed (aHR = 1.68, 95% CI = 1.01–2.79).
TABLE 3.
Hazard Ratios of Time Until Psychiatric Disorders Between Women With Symptomatic Menopausal Transition and Control Subjects During a 10-year Follow-Up Period

DISCUSSION
This is the 1st nationwide retrospective cohort study to examine the association between symptomatic menopausal transition and the risk of subsequent new-onset psychiatric disorders. The major finding of our study is that women with symptomatic menopausal transition may have a higher risk of development of subsequent psychiatric disorders, especially depressive disorder, anxiety disorder, sleep disorder, and bipolar disorder.
Several studies have demonstrated that depression and anxiety are the most common psychiatric symptoms in women with symptomatic menopausal transition. Our study indicated that symptomatic menopausal transition might be a risk factor for subsequent clinical depressive and anxiety disorders. There may be several explanations for this link. First, the withdrawal of hormones may cause a change in the serotonin levels. Estrogens are highly lipophilic hormones that can cross the blood–brain barrier and bind to intracellular estrogen receptors distributed in many organs related to anxiety and depressive disorder, such as the hippocampus.23 In 2009, Walf et al24 found that chronic estradiol replacement in aged female rats reduced anxiety and depressive-like behaviors, suggesting an important role of estradiol in hippocampus-mediated mood regulation. Second, the role of estrogens in the development of anxiety and depressive disorders during menopausal transition may be associated with their neurotrophic and neuroprotective effects. Thus, administration of estradiol to ovariectomized rats induced an increase in the release of brain-derived neurotrophic factor and vascular endothelial growth factor, decreasing depressive-like behavior.25,26 Third, VMS, sexual dysfunction, and obesity,2,27 which are common symptoms in women with symptomatic menopausal transition, have been linked to the development of depressive and anxiety disorders. Last, although most arguments are in favor of a primarily biological rationale, several psychosocial stressors common in mid-life women, such as marital issues, changes in caretaking (children departing home, aging parents) or career responsibilities, issues related to aging, and limited social network have also been linked to depressive and anxiety disorders in women during the menopausal transition.17,28,29 However, the complexity of related social, cultural, psychological, and environmental factors30,31 has resulted in poor understanding of the role of these common psychosocial stressors in the pathogenesis of depression and anxiety in symptomatic menstrual transition.
Our results also indicate that women with symptomatic menopausal transition are at an increased risk of new-onset sleep disorders. Although the hormone changes during menopausal transition are often linked to the development of sleep disturbance, no studies have confirmed the causal relationship between the changes of serum hormone concentrations and the occurrence of sleep disturbance in women during the perimenopausal period. A recent study trying to explore the linkage between the sleep quality and the fluctuation of hormone levels in women revealed that there was no clear relationship between hormone changes and the sleep quality among women during menopausal transition, which implicated that the sleep disturbance during this period may be influenced by other factors, such as emotional disturbance.32 Another study suggested that perimenopausal women with sleep disorders often have VMS and depressive symptoms, which are associated with different patterns of the sleep disorder. For example, depression is uniquely related to difficulty falling asleep and waking up earlier than desired, whereas VMS are related to frequent awakenings during sleep.33
Previous studies reported that progression through the female reproductive stages (premenopause, perimenopause, and postmenopause) is associated with mood course in women with bipolar disorder16 and indicated that such women are at a higher risk of unstable mood episodes during periods of intense hormonal fluctuation such as the menopausal transition. In addition, as long as 3 decades ago, Kukopulos et al19 demonstrated that menopausal transition could induce rapid cycling, whereas Oppenheim20 showed that estrogen induced abruptly rapid mood cycling. These results may further emphasize the important associations between the hormonal changes and bipolar disorders, especially rapid cycling. Moreover, estrogen and progesterone can modulate neurotransmitter systems and intracellular signaling pathways known to be affected by mood-stabilizing agents. In particular, they closely interact with brain-derived neurotrophic factor, oxidative stress, and inflammation pathways, which are involved in the neurobiology of bipolar disorders.34 Although our results indicate that symptomatic menstrual transition might increase the risk of a subsequent newly diagnosed bipolar disorder, no firm conclusions should be drawn at this time given the evidence of high rates of misdiagnosis and delayed treatment of bipolar disorders, especially of type II,35,36 and lack of consistent supporting evidence.
The results of stratification for the duration of follow-up period indicated that the incidences of bipolar disorders, depressive disorders, anxiety disorders, and sleep disorders were increased in the 1st year after the diagnosis of symptomatic menopausal transition. One possible explanation for this result is surveillance bias. Women with symptomatic menopausal transition are likely to have more frequent outpatient visits than the general population, leading to earlier diagnosis of psychiatric disorders. However, as shown in Table 2, the incidences of newly diagnosed bipolar disorders, depressive disorders, anxiety disorders, and sleep disorders remained significantly increased after the 1st year of follow-up, suggesting that the observed effects were not due only to surveillance bias. The present study has several limitations related to the use of a claims database. First, although symptomatic menopausal transition is a clinical diagnosis, data on menstrual cycle as well as results of baseline and longitudinal endocrinological assessments, which could increase the validity of the diagnosis, were unavailable. Second, data on severity of symptomatic menopausal transition and use of hormone replacement therapy were limited. The effects of severity of symptomatic menopausal transition on development of subsequent psychiatric disorders require further investigation. Third, subtypes of psychiatric diagnoses were not specified (eg, bipolar I vs bipolar II, types of depressive disorders, panic vs other anxiety disorders, types of sleep disorders, eg, insomnia vs hypersomnia, delayed or advanced sleep disorder, or restless leg syndrome). Fourth, there was no access to data on personal or family history of psychiatric disorders, and seasonal influences. Fifth, the absence of records on several demographic variables such as domestic environment, lifestyle, and psychosocial stressors represents an additional limitation. Last, the prevalence of psychiatric disorders in our study may be underestimated because only subjects who sought medical evaluation were included. Thus, the risk for a new onset37 or recurrence38 of depressive disorders during the menopausal transition in women with a history of depression has been well documented, and such women may be more likely to attend a menopause clinic.39 The higher possibility of early diagnosis in the study cohort compared to the control cohort was not fully eliminated by the subgroup analysis according to the follow-up duration between the diagnosis of symptomatic menstrual transition and depressive disorder.
In conclusion, symptomatic menopausal transition may be a risk factor for bipolar, depressive, anxiety, and sleep disorders. Although there are several limitations to the claims database study, these limitations are most likely to have a greater influence on the investigated temporal relationship between symptomatic menopausal transition and subsequent psychiatric disorders within the 1st year follow-up. Therefore, based on the results of persistently higher IRRs over longer follow-up periods (1–5 and ≥5 year), symptomatic menopausal transition may play a potential role in new-onset, but not recrudescence of, bipolar, depressive, anxiety, and sleep disorders. However, prospective studies, particularly with additional patient-level data, are warranted to confirm our findings.
Acknowledgments
The authors thank the Research Center of Medical informatics, Kaohsiung Veterans General Hospital and the Economy Company Ltd. for their technical support and academic English editing service. The authors also thank the fund by Kaohsiung Veterans General Hospital, Taiwan (grant numbers VGHKS105-123 and VGHKS105-062) and Yuanshan & Suao Branch, Taipei Veterans General Hospital, Yilan, Taiwan (grant number 104B-001). The study was based on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance of the Department of Health, Taiwan, and managed by the National Health Research Institute, Taiwan. The interpretation and conclusions contained in this article do not represent those of the Bureau of National Health Insurance, the Department of Health, or the National Health Research Institute.
Footnotes
Abbreviations: aHR = adjusted hazard ratio, CI = confidence interval, HR = hazard ratio, ICD-9-CM = the International Classification of Diseases, ninth revision, Clinical Modification, IRR = incidence rate ratio, LHID 2000 = Longitudinal Health Insurance Database 2000, NHI = National Health Insurance, NHIRD = National Health Insurance Research Database, VMS = vasomotor symptoms.
L-YH and C-CS contributed equally to this work.
This study is funded by Kaohsiung Veterans General Hospital, Taiwan (grant numbers VGHKS105-123 and VGHKS105-062) and Yuanshan & Suao Branch, Taipei Veterans General Hospital, Yilan, Taiwan (grant number 104B-001).
The authors have no conflicts of interest to disclose.
REFERENCES
- 1.Kase NG. Impact of hormone therapy for women aged 35 to 65 years, from contraception to hormone replacement. Gend Med 2009; 6 Suppl 1:37–59. [DOI] [PubMed] [Google Scholar]
- 2.McNamara M, Batur P, DeSapri KT. In the clinic. Perimenopause. Ann Intern Med 2015; 162:Itc1–Itc15. [DOI] [PubMed] [Google Scholar]
- 3.Kumari M, Stafford M, Marmot M. The menopausal transition was associated in a prospective study with decreased health functioning in women who report menopausal symptoms. J Clin Epidemiol 2005; 58:719–727. [DOI] [PubMed] [Google Scholar]
- 4.Makara-Studzinska MT, Krys-Noszczyk KM, Jakiel G. Epidemiology of the symptoms of menopause – an intercontinental review. Prz Menopauzalny 2014; 13:203–211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Li S, Holm K, Gulanick M, et al. The relationship between physical activity and perimenopause. Health Care Women Int 1999; 20:163–178. [DOI] [PubMed] [Google Scholar]
- 6.Nelson HD. Menopause. Lancet 2008; 371:760–770. [DOI] [PubMed] [Google Scholar]
- 7.NIH State-of-the-Science Conference Statement on management of menopause-related symptoms. NIH Consens State Sci Statements 2005; 22:1–38. [PubMed] [Google Scholar]
- 8.Borkoles E, Reynolds N, Thompson DR, et al. The role of depressive symptomatology in peri- and post-menopause. Maturitas 2015; 81:306–310. [DOI] [PubMed] [Google Scholar]
- 9.Du HG, Ming L, Chen SJ, et al. Xiaoyao pill for treatment of functional dyspepsia in perimenopausal women with depression. World J Gastroenterol 2014; 20:16739–16744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Marsh WK, Templeton A, Ketter TA, et al. Increased frequency of depressive episodes during the menopausal transition in women with bipolar disorder: preliminary report. J Psychiatr Res 2008; 42:247–251. [DOI] [PubMed] [Google Scholar]
- 11.Sajatovic M, Friedman SH, Schuermeyer IN, et al. Menopause knowledge and subjective experience among peri- and postmenopausal women with bipolar disorder, schizophrenia and major depression. J Nerv Ment Dis 2006; 194:173–178. [DOI] [PubMed] [Google Scholar]
- 12.Jafari F, Hadizadeh MH, Zabihi R, et al. Comparison of depression, anxiety, quality of life, vitality and mental health between premenopausal and postmenopausal women. Climacteric 2014; 1–6. [DOI] [PubMed] [Google Scholar]
- 13.Tom SE, Kuh D, Guralnik JM, et al. Self-reported sleep difficulty during the menopausal transition: results from a prospective cohort study. Menopause 2010; 17:1128–1135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gupta R, Assalman I, Bottlender R. Menopause and schizophrenia. Menopause Int 2012; 18:10–14. [DOI] [PubMed] [Google Scholar]
- 15.Seeman MV. Treating schizophrenia at the time of menopause. Maturitas 2012; 72:117–120. [DOI] [PubMed] [Google Scholar]
- 16.Marsh WK, Ketter TA, Crawford SL, et al. Progression of female reproductive stages associated with bipolar illness exacerbation. Bipolar Disord 2012; 14:515–526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Marsh WK, Templeton A, Ketter TA, et al. Increased frequency of depressive episodes during the menopausal transition in women with bipolar disorder: preliminary report. J Psychiatr Res 2008; 42:247–251. [DOI] [PubMed] [Google Scholar]
- 18.Freeman MP, Smith KW, Freeman SA, et al. The impact of reproductive events on the course of bipolar disorder in women. J Clin Psychiatry 2002; 63:284–287. [DOI] [PubMed] [Google Scholar]
- 19.Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic-depressive cycle and changes caused by treatment. Pharmakopsychiatr Neuropsychopharmakol 1980; 13:156–167. [DOI] [PubMed] [Google Scholar]
- 20.Oppenheim G. A case of rapid mood cycling with estrogen: implications for therapy. J Clin Psychiatry 1984; 45:34–35. [PubMed] [Google Scholar]
- 21.Wu CY, Chen YJ, Ho HJ, et al. Association between nucleoside analogues and risk of hepatitis B virus-related hepatocellular carcinoma recurrence following liver resection. JAMA 2012; 308:1906–1914. [DOI] [PubMed] [Google Scholar]
- 22.Avis NE, Crawford SL, Greendale G, et al. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med 2015; 175:531–539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ostlund H, Keller E, Hurd YL. Estrogen receptor gene expression in relation to neuropsychiatric disorders. Ann N Y Acad Sci 2003; 1007:54–63. [DOI] [PubMed] [Google Scholar]
- 24.Walf AA, Paris JJ, Frye CA. Chronic estradiol replacement to aged female rats reduces anxiety-like and depression-like behavior and enhances cognitive performance. Psychoneuroendocrinology 2009; 34:909–916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Licht T, Goshen I, Avital A, et al. Reversible modulations of neuronal plasticity by VEGF. Proc Natl Acad Sci U S A 2011; 108:5081–5086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Warner-Schmidt JL, Duman RS. VEGF is an essential mediator of the neurogenic and behavioral actions of antidepressants. Proc Natl Acad Sci U S A 2007; 104:4647–4652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Blumel JE, Chedraui P, Aedo S, et al. Obesity and its relation to depressive symptoms and sedentary lifestyle in middle-aged women. Maturitas 2015; 80:100–105. [DOI] [PubMed] [Google Scholar]
- 28.Sajatovic M, Friedman SH, Schuermeyer IN, et al. Menopause knowledge and subjective experience among peri- and postmenopausal women with bipolar disorder, schizophrenia and major depression. J Nerv Ment Dis 2006; 194:173–178. [DOI] [PubMed] [Google Scholar]
- 29.Johansson L, Guo X, Hällström T, et al. Common psychosocial stressors in middle-aged women related to longstanding distress and increased risk of Alzheimer's disease: a 38-year longitudinal population study. BMJ Open 2013; 3:e003142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bauld R and RF, Brown RF. Stress, psychological distress, psychosocial factors, menopause symptoms and physical health in women. Maturitas 2009; 62:160–165. [DOI] [PubMed] [Google Scholar]
- 31.Kuh D, Hardy R, Rodgers B, et al. Lifetime risk factors for women's psychological distress in midlife. Soc Sci Med 2002; 55:1957–1973. [DOI] [PubMed] [Google Scholar]
- 32.de Zambotti M, Colrain IM, Baker FC. Interaction between reproductive hormones and physiological sleep in women. J Clin Endocrinol Metab 2015; jc20143892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Xu Q, Lang CP. Examining the relationship between subjective sleep disturbance and menopause: a systematic review and meta-analysis. Menopause 2014; 21:1301–1318. [DOI] [PubMed] [Google Scholar]
- 34.Frey BN, Dias RS. Sex hormones and biomarkers of neuroprotection and neurodegeneration: implications for female reproductive events in bipolar disorder. Bipolar Disord 2014; 16:48–57. [DOI] [PubMed] [Google Scholar]
- 35.Oyffe I, Shwizer R, Stolovy T. The association between diagnosis, treatment delay and outcome among patients with bipolar disorders. Psychiatr Q 2015; 86:95–105. [DOI] [PubMed] [Google Scholar]
- 36.Angst J. The emerging epidemiology of hypomania and bipolar II disorder. J Affect Disord 1998; 50:143–151. [DOI] [PubMed] [Google Scholar]
- 37.Chen MH, Su TP, Li CT, et al. Symptomatic menopausal transition increases the risk of new-onset depressive disorder in later life: a nationwide prospective cohort study in Taiwan. PLoS One 2013; 8:e59899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Clayton AH, Ninan PT. Depression or menopause? Presentation and management of major depressive disorder in perimenopausal and postmenopausal women. Prim Care Companion J Clin Psychiatry 2010; 12 1: PCC.08r00747. doi:10.4088/PCC.08r00747blu. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hay AG, Bancroft J, Johnstone EC. Affective symptoms in women attending a menopause clinic. Br J Psychiatry 1994; 164:513–516. [DOI] [PubMed] [Google Scholar]