

Summary
Tourette syndrome is a chronic neurodevelopmental disorder characterised by motor and phonic tics that can substantially diminish the quality of life of affected individuals. Evaluating and treating Tourette syndrome is complex, in part due to the heterogeneity of symptoms and comorbidities between individuals. The underlying pathophysiology of Tourette syndrome is not fully understood, but recent research in the past 5 years has brought new insights into the genetic variations and the alterations in neurophysiology and brain networks contributing to its pathogenesis. Treatment options for Tourette syndrome are expanding with novel pharmacological therapies and increased use of deep brain stimulation for patients with symptoms that are refractory to pharmacological or behavioural treatments. Potential predictors of patient responses to therapies for Tourette syndrome, such as specific networks modulated during deep brain stimulation, can guide clinical decisions. Multicentre data sharing initiatives have enabled several advances in our understanding of the genetics and pathophysiology of Tourette syndrome and will be crucial for future large-scale research and in refining effective treatments.
Introduction
Tourette syndrome, named after and described by Georges Gilles de la Tourette in 1885,1 is a childhood-onset neurodevelopmental disorder characterised by involuntary movements (motor tics) and vocalisations (phonic tics). An estimated 0·3–0·9% of school-aged children (4–18 years)2 and 0·002–0·08% of adults3 have a diagnosis of Tourette syndrome, although few adult epidemiological studies have been done globally. Tourette syndrome occurs more frequently in males, with a male-to-female ratio of 4:1, and males tend to have more severe symptoms than females.4 Tourette syndrome is often accompanied by comorbid behavioural disorders, including most prominently obsessive-compulsive behaviour and attention deficit disorders.
Diagnosis and treatment of and research into Tourette syndrome and its associated comorbidities is complex. Symptoms and comorbidities severities are highly heterogeneous, and fluctuate over time. Although the pathophysiology of Tourette syndrome is not fully understood, various genetic and neurophysiological factors are likely to contribute. Established treatments for Tourette syndrome include behavioural therapies and medications, and emerging treatments include non-invasive neuromodulation and deep brain stimulation. Many gaps in knowledge about Tourette syndrome remain, including the factors contributing to the variability in clinical manifestations and how to best treat tics and comorbidities. In this Review, we provide an overview of the latest evidence on the clinical features, diagnosis, genetics, pathophysiology, and treatment of Tourette syndrome. In particular, recent progress in the past 5 years has been made in refining the pathophysiological models and genetics of Tourette syndrome, and in the further development of pharmacological, behavioural, and neuromodulation interventions. We also highlight key questions and topics for future research.
Clinical features and diagnosis
Motor and phonic tics
Motor and phonic tics, the hallmark symptoms of Tourette syndrome, vary widely between individuals in type, severity, frequency, and complexity (figure 1). Tics are generally categorised into simple and complex, and they can include virtually any combination of movements or vocalisations. Simple motor tics are brief repetitive movements that involve a single muscle group or body part (eg, blinking and snapping fingers), whereas complex motor tics are distinct coordinated patterns of movements involving multiple muscle groups (eg, facial grimace with a head tilt and a shoulder shrug, and spinning around while walking). Simple phonic tics are non-word vocalisations (eg, sniffing, single syllables, or noises), and complex phonic tics include phrases or combinations of sounds. Obscene or socially inappropriate gestures or vocalisations (coprophenomena) occur in approximately 28·1% of individuals with Tourette syndrome.5 The severity of tics has been documented to worsen under stress, fatigue, or excitement, and to improve when the individual is engaged in mental or physical activity, or during focused attention.6,7 Tics can be involuntary or semi-voluntary (ie, voluntary responses to urges or sensory phenomena), and in some cases, the distinction between the two can be challenging even for an experienced clinician.8 Premonitory urges often precede tics, although an observational study of 21 adults with Tourette syndrome suggested that tics have a consistent temporal association with premonitory urges in only 57–66% of individuals, depending on the method used to measure the urges.9 Tics can sometimes be partly or completely suppressed, although the ability to suppress tics varies between individuals.10 Furthermore, according to a retrospective study of 201 patients with Tourette syndrome, 17% of individuals with Tourette syndrome experience self-injurious tics.11 In extreme cases, self-injurious tics can lead to injury necessitating hospitalisation, loss of bodily function, or permanent disfigurement.12
Figure 1. Variability of Tourette syndrome and associated comorbidities.

(A) Child with common simple motor and phonic tics (eg, shrugging shoulders and winking). (B) Adolescent with a combination of complex motor tics (eg, pulling hair) and complex phonic tics (eg, saying “donť trip”), and emerging behavioural features including attention deficit hyperactivity disorder (ADHD) depicted as swirling thoughts. (C) Although tics become less severe after adolescence in most cases, complex motor tics, phonic tics, and behavioural features can persist into adulthood in some individuals. This adult example experiences complex motor tics (eg, hand gestures, followed by snapping fingers and scatching their head) and phonic tics (eg, humming repetitively). (D) Psychiatric and behavioural comorbidities can be the primary symptoms (with or without tics) in some individuals and can include obsessive-compulsive disorder (eg, checking behaviours, as depicted in the thought cloud) or mood disorders (eg, depression or anxiety, depicted as darkness in the thought cloud). Although individuals of various ages are depicted, tics and comorbidities do not follow a single time course; the natural history of Tourette syndrome and the severities and types of symptoms differ widely among patients of various ages.
Diagnosis and evaluation
Tourette syndrome is diagnosed through clinical assessment using the individual's history. The American Psychiatric Diagnostic and Statistical Manual of Mental Disorders (DSM-5) specifies that to diagnose Tourette syndrome, tics must have begun before the age of 18 years and the individual must have had tics for at least 1 year, including at least two motor tics and one phonic tic. DSM-5 differentiates between provisional tic disorders, persistent (chronic) tic disorders, and Tourette syndrome; however, defining these disorders as a spectrum (listed from least to most severe) has been proposed.13,14 Family history of tics or Tourette syndrome can also aid in diagnosis, but it is not a requirement.
Several rating scales can be used for evaluation of symptoms in individuals with Tourette syndrome of any age group,15 but the Yale Global Tic Severity Scale (YGTSS) is the most commonly used tool. Given the variability and fluctuations in symptoms, guidelines16 recommend using multiple methods for measuring symptom severity, including direct observation in environments within and outside the clinic, historical information from the individual and their family, and video-based assessment.
Diagnosis and evaluation of Tourette syndrome can be challenging due to its clinical heterogeneity, the suppressibility of tics, and symptom fluctuations over time and under different conditions. Diagnosis can be delayed up to 3–11 years after symptom onset, and an estimated 73% of patients receive an initial misdiagnosis, although this estimate is based on patient self-report, which shows the low awareness and knowledge in the general community and among health professionals of how to recognise Tourette syndrome.17,18 Early diagnostic markers, such as imaging, blood, or CSF biomarkers, have not yet been identified to enable diagnosis before symptoms emerge. However, some evidence suggests individuals with particular characteristics are at risk of developing tics. For example, a study by a multicentre consortium suggests that children with conduct problems, autism spectrum disorder symptoms, compulsions, and emotional problems might be more at risk of developing tics.19 Increasing awareness about Tourette syndrome and its risk factors could enable caregivers and health-care providers to recognise tics and establish treatment early.
Accurate diagnosis of Tourette syndrome can be challenging due to the presence of other behavioural disorders20,21 and difficulty in differentiating between tics and functional tic-like behaviours.22 During the COVID-19 pandemic, there has been a worldwide increase in adolescents and young adults presenting with functional tic-like behaviours linked to watching videos on social media of individuals executing movements and vocalisations meant to depict symptoms of Tourette syndrome.23,24 Functional tic-like behaviours differ from Tourette syndrome by an abrupt and later onset of symptoms, an absence of symptom fluctuations, a higher prevalence in females than males, and more complex motor and vocal tics.23,24 Early and accurate diagnosis and treatment of Tourette syndrome is crucial because symptoms can interfere with social integration and cognitive and intellectual development, and treatment can mitigate symptoms and reduce challenges in daily life for the affected individual and caregivers.
Time course of symptoms
The time course of Tourette syndrome is variable. Tics typically start in individuals aged 3–8 years, often beginning with simple motor tics (figure 1) followed by phonic tics. The peak severity of tics is commonly in individuals aged 8–12 years (mean [SD] of 10 [2·4] years).25 A single centre study5 of 1032 individuals has reported that premonitory urges and the ability to suppress tics can also be present from around tic onset. The severity of tics and most associated psychiatric disorders typically improve with age.26 However, a prospective longitudinal follow-up study of 314 individuals with Tourette syndrome27 has suggested that only 17% of patients will experience complete remission after the age of 16 years, and 60% will still experience some persistent mild to moderate tics. Up to 23% of affected individuals will have persistent and, in some cases, severe tics into adulthood (figure 1).27
Predictors of the time course of Tourette syndrome have not been well established and few longitudinal large cohort studies have been done. Childhood tic severity28 (but not age at tic onset5), a family history of Tourette syndrome, presence of comorbidities, teasing in childhood perhaps due to symptoms, and psychosocial stress might predict tic severity into early adulthood.28,29 Identification of predictors of who will experience severe symptoms into adulthood will be crucial to enable the development of effective treatment plans and ensure that these individuals receive the support they need as adults.
Comorbidities
Tourette syndrome commonly occurs with other psychiatric and behavioural disorders, including obsessive-compulsive behaviour or obsessive-compulsive disorder (OCD), attention-deficit hyperactivity disorder (ADHD), autism spectrum disorder, anxiety, depression, sleep disorders, and self-injurious behaviour.5 A cross-sectional study in 1374 individuals suggests that isolated Tourette syndrome is the exception, not the rule: up to 88% of individuals with Tourette syndrome are diagnosed with at least one additional psychiatric disorder during their lifetime and 58% are diagnosed with two or more comorbidities (figure 1).30 The most common comorbidities are ADHD and OCD, with an estimated 72% of individuals with Tourette syndrome diagnosed with either disorder.30
Although timelines vary among individuals, ADHD might have the earliest onset (median age 5 [IQR 3–6] years), followed by OCD (7 [5–9] years), anxiety disorders (7 [4–10] years), and mood disorders (13 [10–18] years).30 Additionally, consistent with other psychiatric disorders, individuals with Tourette syndrome and comorbidities have increased risk of mortality by natural or unnatural causes (such as suicide) when compared with individuals with Tourette syndrome without comorbidities, although the contributing factors are unclear.31 Assessments for comorbid behavioural and psychiatric symptoms in children with Tourette syndrome should begin early and be repeated at regular intervals, as comorbidities generally have a greater detrimental effect on quality of life than tic severity.32
Genetics
Tic disorders are considered to be among the most heritable neuropsychiatric disorders. Two large population-based and genome-wide association studies (approximately 4800 individuals in each) have estimated that genetic variants explain 77·0–92·4% of the heritability of Tourette syndrome, with similar risk in males and females.33,34 Although the DSM-5 diagnostic criteria differentiate between Tourette syndrome and chronic tic disorders, studies suggest both disorders result from a similar genetic background.34,35
Among familial factors, parental and especially maternal psychiatric diagnoses have been associated with a diagnosis of Tourette syndrome in offspring.36 Indeed, large studies on neurological and psychiatric disorders showed a high genetic correlation among psychiatric disorders, suggesting important overlap in common gene variants that might explain why individuals with psychiatric disorders, particularly those with Tourette syndrome, have an increased risk of developing OCD and major depressive episodes.37,38
One study using whole exome sequencing of 511 Tourette syndrome trios (affected children and both biological parents) showed that in approximately 12% of individuals with Tourette syndrome, de novo damaging gene variants contributed to the risk of the disorder and there was no difference across sexes.39 A study of 222 trios of children with OCD and their parents showed these de novo variants account for 22% of cases of OCD.40 However, not one of the genes implicated in Tourette syndrome has met the threshold for high-confidence association for both Tourette syndrome and OCD, which suggests that specific neuronal pathways for these disorders exist.40 The cause of Tourette syndrome is monogenetic in less than 2% of individuals; the genes that cause monogenetic Tourette syndrome include genes implicated in neuronal and dendrite development, axonal guidance, cellular membrane stability (eg, SLITRK 1–6, CELSR3, CNTN6, and NRXN1),34 neurotransmitters such as opioids (OPRK1),41 and histamine (histidine decarboxylase (HDC) genes).42 Because the population with Tourette syndrome related to monogenetic causes is small, generalisation of findings from these individuals to the whole Tourette syndrome population is difficult.
Although genetic and familial factors probably affect brain pathway development and the manifestation of Tourette syndrome, the exact mechanisms of these interactions are unclear. However, whole exome studies have implicated some cellular processes in Tourette syndrome pathophysiology, including genes regulating cell polarity and migration,39,43 cell adhesion molecules implicated in trans-synaptic signalling, ion channel signalling through GABA and glutamate neurotransmitters, glial-derived neuroimmunity,44 and synaptic membrane stability.45 A meta-analysis of genome-wide cell and tissue-based enrichment analyses in a database of 714 healthy adult donors with samples collected from 53 distinct human tissues (from the brain and elsewhere) revealed that modulation of expression of numerous genes through non-coding variants might be a key mechanism in Tourette syndrome pathogenesis, with the brain regions most affected by genes implicated in Tourette syndrome being the dorsolateral prefrontal cortex, followed by frontal cortex, striatum, and cerebellum.34
New advancements in our understanding of neuroimmunity are of particular interest for Tourette syndrome because neurodevelopmental deficits might result both from external factors, such as maternal inflammation leading to fetal neuroinflammation,46,47 and from perturbation of genetic neuroimmunological pathways as a result of genetic variants.44 Some peripheral markers, such as myeloid type 1 and 2 cells, implicated in the pathogenesis of autoimmune disorders, also support the alteration of the immune-brain crosstalk in Tourette syndrome, suggesting that immunomodulation might be a promising avenue for treatment.48
Pathophysiology
Convergent evidence drawn from both genetics and neuroimaging strongly supports that Tourette syndrome is a neurodevelopmental disorder. Neuroimaging studies have revealed a difference in functional brain connectivity (ie, a statistically significant measure of brain activity derived from functional imaging in the at-rest condition) when comparing adults who have Tourette syndrome with children who have Tourette syndrome.49 Additionally, developmental trajectories seemed to differ in individuals with Tourette syndrome, in which the functional brain connectivity of children with Tourette syndrome appeared older, and the functional brain connectivity of adults with Tourette syndrome appeared younger, when compared with age-matched controls.49 This difference might result from variances in cellular and axonal pruning, potentially influenced by genetic and environmental factors.50 Collectively, genetic and environmental factors are likely to result in widespread neuronal network dysfunction and the potential emergence of symptoms related to Tourette syndrome (figure 2).53, 54
Figure 2. Models of Tourette syndrome pathophysiology.

(A) Cortico-basal ganglia networks and Tourette syndrome clinical characteristics. Distinct cortico-basal ganglia networks are related to tics (sensorimotor network [orange]) and comorbidities (associative and limbic networks [grey]) in Tourette syndrome. (B) Neuropathological underpinnings of Tourette syndrome: stereological cellular count in post-mortem tissue revealed different cellular distributions in the basal ganglia of individuals with Tourette syndrome (3 patients, mean [SEM] age 42·0 [11·9] years) compared with controls (5 healthy controls, mean [SEM] age 60·0 [9·7] years; left panel), with fewer inhibitory GABAergic cells (red circle) and cholinergic cells (green hexagon) within the striatum in Tourette syndrome (5 patients, mean [SEM] age 43·0 [3·6] years) compared with 5 controls mean [SEM] age 61·8 [4·3] years (right panel). (C) Model of relationship between premonitory urges and tics: abnormal interoceptive information processing (insular cortex; blue area) and exteroceptive processing (sensorimotor cortex; pink areas) results in genesis of premonitory urges (insular cortex), leading to action initiation (via anterior cingulate cortex; green area) and subsequent tic execution (via cortico-basal ganglia sensorimotor network (as shown in A). Acc=anterior cingulate cortex. Ach+=cholinergic interneurons of the striatum. ADHD=attention deficit hyperactivity disorder. GABA Pav+=GABAergic parvalbumin-positive interneurons of the striatum. GPi=globus pallidus internus. GPe=globus pallidus externus. Ins=insular cortex. MSN=medium spiny neurons. OCD=obsessive-compulsive disorder. OFC=orbitofrontal cortex. SM=sensorimotor cortex. B (left) has been adapted from Kalanithi and colleagues51 and B (right) from Kataoka and colleagues52.
On a network level, tics might be a product of inhibitory dysfunction within the sensorimotor cortico-basal ganglia network,55 namely from alterations of striatal inhibitory microcircuitry (figure 2)51,52,53,54,55,56 and problems with automatic inhibition of actions.57 This inability to delay an action has been correlated with the severity of tics.58 In contrast, volitional inhibition, measured by proactive inhibition (inhibition of action in preparation) or reactive inhibition (inhibition of already initiated action), is largely unaltered in people with Tourette syndrome,59 and has been related to the individual's capacity to inhibit their tics.60
However, the disinhibition model does not explain some fundamental features of tic disorders, such as the waxing and waning character and the premonitory urges. An alternative hypothesis is that tics could represent exaggerated and persistent motor habits that are reinforced by aberrant increased phasic dopamine release.61 In support of this idea, dopamine-associated reward-guided learning, also known as reinforcement learning, seems to be enhanced in Tourette syndrome.62 Individuals with Tourette syndrome tend to rely on habits when in the non-medicated state.63 Therefore, the hypothesis that aberrant tonic dopamine release increases the execution of learned actions (ie, tics), via changes of plasticity in the direct and indirect cortico-basal ganglia pathways, has gained some traction.61 Tics as a habitual and learned action also might explain premonitory urges: termination of premonitory urges by execution of tics might trigger a positive prediction error and phasic dopamine release, thus reinforcing the learning of tics.64 The current model of premonitory urges (figure 2) proposes that abnormal interoceptive and exteroceptive processing might generate premonitory urges, leading to action initiation and subsequent tic execution via the cortico-basal ganglia sensorimotor network.65
Neurophysiological studies in humans can identify markers of tics during surgery to implant deep brain stimulation devices,66 during externalised lead studies,67 or via neurostimulators capable of recording neural activity.68,69,70 All of these studies point to increased activity in low-frequency power (1–10 Hz) in the centromedian thalamic region in individuals with Tourette syndrome that might be associated with tics (appendix). Other studies also have revealed the presence of low-frequency activity in the anterior pallidum in Tourette syndrome.67,71,72,73 How this low-frequency activity translates into tics is unclear, but low-frequency power in the anterior pallidum might be associated with premonitory urges.74
Additional alternative hypotheses related to Tourette syndrome pathogenesis include Tourette syndrome being a disorder of social behavioural networks.75 This hypothesis could explain the common predominant eye, face, and head distribution of tics. Face perception in Tourette syndrome was shown to elicit abnormally high activity compared with healthy controls in the insular cortex and the neural network implicated in tic generation, including motor cortical regions and the putamen.76 Another important clue was provided in a study of sensory perception–action binding, showing increased strength of binding between perception and action in Tourette syndrome compared with healthy controls, which was also correlated with severity of tics. Analysis of EEG signals during an event file coding task to measure perception-action binding showed that this effect was associated with activity in the inferior parietal cortex, suggesting that tics could be an elicited response to internal or even external stimuli.77
Treatments
Treatments approved for Tourette syndrome include behavioural therapies, and pharmacological therapies, or a combination of the two. Research is ongoing to develop and refine new effective treatments for Tourette syndrome, including non-invasive neuromodulation modalities and deep brain stimulation, although neither are currently approved for clinical use. In this section, we present the latest evidence and summarise guidelines for Tourette syndrome therapies, from first-line therapies to therapies reserved for select patients with severe, treatment-refractory symptoms.
Behavioural therapies
Comprehensive Behavioural Intervention for Tics (CBIT) is rated as effective in tic reduction in both children and adults with Tourette syndrome according to guidelines from the American Academy of Neurology (AAN)78,79 and the European Society for the Study of Tourette Syndrome (ESSTS).80 Notably, CBIT is the only therapy in the AAN guidelines with high confidence in its efficacy (panel). CBIT is recommended as an initial treatment option before the initiation of pharmacotherapy or other non-pharmacological interventions. Overall, CBIT has been reported to reduce the number and severity of tics by 26–31% as measured by the YGTSS across studies. One randomised control trial in 110 patients (aged 8–17 years) suggested that it was as effective as pharmacological treatment.82
Panel:
Overview of therapies for Tourette syndrome
| Behavioral therapies: |
|---|
| • Comprehensive behavioral intervention for tics and habit reversal training* |
| • Exposure and response prevention† |
| Pharmacological therapies: |
| First-line |
| • Atypical antipsychotics (ie, aripiprazole‡, tiapride‡, and risperidone‡) |
| Second-line |
| • Typical antipsychotics (ie, haloperidol‡ and pimozide§) |
| • Anticonvulsants (ie, topiramate§) |
| • Antidepressants (ie, desipramine§) |
| • Chinese medicine (ie, Ningdong granule‡ and 5-Ling granule‡) |
| • Neurotoxins (ie, Botulinum toxin injections‡ [focal tics]) |
| Neuromodulation therapies (for patients with severe, treatment-refractory symptoms): |
| • Deep brain stimulation targeted to the pallidum† or the thalamus† |
| • Transcranial magnetic stimulation† targeted to the supplementary motor area, primary motor area, or prefrontal cortex |
| Therapies that could have therapeutic effects on tics and comorbidities: |
| • Tourette syndrome plus obsessive-compulsive disorder: cognitive behavioral therapy (eg, exposure and response prevention) or selective serotonin reuptake inhibitors¶ |
| • Tourette syndrome plus attention deficit hyperactivity disorder: clonidine‡ and guanfacine§ |
The above therapy types are presented in order of suggested use according to guidelines from the American Academy of Neurology (AAN)78,79 and the European Society for the Study of Tourette Syndrome (ESSTS).80,81 First-line and second-line designations for pharmacological therapies were assigned according to the ESSTS guidelines.80 Evidence levels were determined according to a modified form of the Grading of Recommendations Assessment, Development, and Evaluation process according to the AAN comprehensive review.79
Evidence level is high.
Insufficient evidence of efficacy.
Evidence level is moderate.
Evidence level is low.
Not evaluated as part of the AAN comprehensive review, but discussed as potentially effective in the ESSTS guidelines.
Habit reversal training is one of the main components of CBIT. Habit reversal training aims to increase a person's awareness of premonitory urges and tics. Another component of CBIT focuses on competing response training, which is used in an effort to suppress tics.83,84 If CBIT is unavailable, exposure and response prevention, which suppresses tics gradually over time,85 can be tried to increase the tolerance to premonitory urges and to potentially reduce tics.78 Alternating between habit reversal training and exposure and response prevention might be valuable, although there is only one randomised trial in 54 adolescents (aged 9–17 years).86 Group therapy has also been suggested as a practical and cost effective alternative for children and adolescents.87 Videoconference88 and telemedicine approaches89 might be similarly effective to in-person behavioural therapies and will likely improve access for patients and their caregivers.
Although behavioural therapies are effective for many individuals with Tourette syndrome, some patients might not benefit from them. Thus, several studies have focused on identifying predictors and moderators of good response to behavioural therapy. In an analysis of data from clinical trials assessing the efficacy of CBIT and psychoeducation and supportive therapy (PST), ADHD, OCD, and anxiety did not significantly moderate the tic severity reduction obtained with CBIT; however, anxiety disorders and premonitory urge severity were associated with less reduction in tic severity across CBIT or PST.90 This analysis also revealed that tic suppressing medication might moderate CBIT effectiveness, and CBIT might be more effective for individuals who are medication naive compared to those who have tried medication.90 However, questions remain about the optimal age to implement CBIT and differences in effects among individuals using different medications. Further research is needed to disentangle the factors contributing to the clinical response to behavioural therapy for Tourette syndrome.
Pharmacological treatments
Pharmacological treatments are suggested for individuals for whom behavioural therapies have not been effective or are unavailable, and for those with severe tics that require more urgent treatment. Several pharmacological treatments have been evaluated to reduce tics, including α2-agonists, typical and atypical antipsychotics, and anticonvulsants.
The evidence for efficacy and adverse effects of pharmacological treatments was recently reviewed by the AAN and by the ESSTS in the past 3 years.78,79,81 According to the AAN, no pharmacological treatments warranted high confidence in their efficacy for tic reduction, probably due to the relative paucity of rigorous clinical trials. However, the ESSTS suggested a hierarchy for selecting medications based on evidence and a survey among Tourette syndrome specialists. We have combined the complementary reports from both organisations to summarise a suggested order for pharmacological treatments and their respective amount of evidence for tics and for individuals with comorbid ADHD or OCD (panel).81 We highlight the pharmacological agents deemed beneficial with moderate or low confidence for benefit based on the AAN guidelines and latest evidence.78,79 The survey administered to 59 Tourette syndrome specialists as part of the ESSTS guidelines indicated that medication preferences did not substantially differ for adults versus children and adolescents. Aripiprazole was the most common choice for all age groups; however, haloperidol was more commonly considered in adults than in children, and tiapride was more often considered in children and adolescents than in adults.81
Although pharmacological treatments can be highly successful for managing symptoms, many patients might not experience therapeutic effects or might have adverse effects. Thus, several new pharmacological compounds are being examined for use in Tourette syndrome. Ecopipam, a dopamine D1-receptor antagonist, was tested in a double-blind randomised trial on 40 patients with Tourette syndrome (aged 7–17 years) and showed significant improvement of total tic scores with an overall safe profile with regards to adverse effects and dropout rate.91 Further double-blind randomised studies are needed to assess the effect of ecopipam on tics and Tourette syndrome. Neither the AAN78,79 or the ESSTS81 addressed this compound in their guidelines. Valbenazine, a vesicular monoamine transporter inhibitor, was tested in several clinical trials for paediatric and adult Tourette syndrome. A randomised study in both children and adults did not show a benefit over placebo treatment,92 despite previous encouraging open-label trials and reports. One open-label trial revealed a positive effect of another vesicular monoamine transporter inhibitor, deutetrabenazine, on tics in adolescents (aged 12–18 years);93 however, a placebo-controlled randomised study did not show benefit.94
The positive effect of cannabinoids for Tourette syndrome in adults has been shown in open label trials.95,96 One retrospective data analysis of cannabis compounds revealed a self-reported improvement of tics and an overall positive adverse-effect profile.95 However, several systematic reviews and meta-analyses have not revealed robust effects on tic suppression.97,98,99 The double-blinded CANNA-TICS trial investigated the capacity of nabiximols, drugs combining a standardised dose of tetrahydrocannabinol and cannabidiol compounds, as a possible approach to reduce tic frequency and severity in adults.100 Preliminary results from this study reported during the 2021 ESSTS conference showed an absence of effect compared with placebo, but the final results are awaited. Accordingly, the AAN78,79 and the ESSTS81 guidelines categorised the treatment with cannabis compounds as experimental that might be given to patients with otherwise treatment-resistant Tourette syndrome.
Non-invasive neuromodulation
Several clinical trials have investigated non-invasive brain stimulation of motor cortical areas (motor cortex and supplementary motor area), including transcranial direct current stimulation or repetitive transcranial magnetic stimulation, in both adults and children with Tourette syndrome. The underlying rationale for transcranial direct current stimulation or repetitive transcranial magnetic stimulation is to modulate pathological neural activity in brain networks implicated in Tourette syndrome to improve symptoms. Overall, these techniques were considered safe. In clinical studies, the results have been conflicting with some studies reporting improvement of tics and associated OCD whereas others have reported no benefit.101,102,103 The inconsistencies might be attributable to the differences in stimulation protocols and the possible influence of comorbidities, such as ADHD, on cortical excitability. The current AAN guidelines and the European guidelines for treatment of Tourette syndrome do not recommend non-invasive brain stimulation for the treatment of tics.
In addition to non-invasive brain stimulation, there is increasing interest in other non-invasive neuromodulation modalities for Tourette syndrome to improve tics. One study showed that, in 20 adolescents and adults with Tourette syndrome, rhythmic peripheral somatosensory stimulation of the median nerve modified the activity (measured by EEG) of the motor cortex, and reduced tic frequency and intensity.104 There was a long-lasting post-stimulation effect in some individuals; however, much larger cohorts will be required to verify these results. Additionally, there has been a single randomised sham-controlled study investigating real-time functional MRI neurofeedback to improve tics.105 This study directed visual modulation of the activity of the supplementary motor area as a treatment for tics in adolescents (21 patients aged 11–19 years). There was a clinically meaningful effect of this intervention on tics when compared with the sham-controlled study, but it is unclear whether the therapy will be practical or sustained.
Deep brain stimulation
Deep brain stimulation is a promising neurosurgical treatment for carefully selected individuals with severe, treatment-refractory Tourette syndrome.106 It is not approved by the US Food and Drug Administration or regulatory agencies in other countries. However, over 300 patients worldwide have been treated with deep brain stimulation according to the Tourette Association of America International Tourette Syndrome Deep Brain Stimulation Registry and Database. Overall, the safety profile of deep brain stimulation for Tourette syndrome is favourable when executed by an experienced multidisciplinary team.107 Improvements in tics and comorbidities have been shown in numerous open-label and retrospective studies, which make up most of the evidence to date. Multicentre retrospective studies and meta-analyses have reported mean improvements of 45·1–52·7% in tic severity in retrospective studies, the largest of which included 185 patients.107,108,109,110 Outcomes across the few randomised controlled trials, which have been done only in adults, have been mixed and difficult to generalise due to small sample sizes and differences in study design.111,112,113,114 The mixed results across trials highlight the challenges of implementing randomised trials in the Tourette syndrome population and the importance of stringent patient selection and of allowing time for stimulation parameter optimisation in a fluctuating disease.
The most common brain targets for deep brain stimulation in Tourette syndrome are the centromedian thalamic region and the anteromedial or posteroventral regions of the pallidum (panel). Previous multicentre studies and meta-analyses have shown similar tic improvement with thalamic versus pallidal deep brain stimulation.107,108,109 However, one meta-analysis revealed greater improvement in tics and obsessive-compulsive behaviour with pallidal deep brain stimulation,115 and the AAN guidelines reported moderate confidence that pallidal deep brain stimulation reduces tic severity (panel).79 There is no clear consensus on which target is most effective for improving tics; however, similar to more commonly treated disorders like Parkinson's disease, individual symptom profiles and comorbidities might be important factors when selecting the optimal surgical target for a given patient with Tourette syndrome. For example, a retrospective study of 55 patients from a single centre found anteromedial pallidum stimulation led to greater improvement in OCD symptoms than did thalamic stimulation.116 Other studies suggest that the structural networks modulated by deep brain stimulation that are associated with tic improvement might differ across surgical targets. Tic improvement with deep brain stimulation targeted to either the anteromedial or posteroventral pallidum was associated with modulation of limbic and associative structural networks, and improvement with thalamic stimulation was associated with sensorimotor networks (figure 3).117,118,119,120,121 Larger multicentre studies are necessary to develop specific predictors to optimise patient-tailored brain target selection.
Figure 3. Neurosurgical targets for deep brain stimulation in Tourette syndrome and structural networks associated with tic improvement.
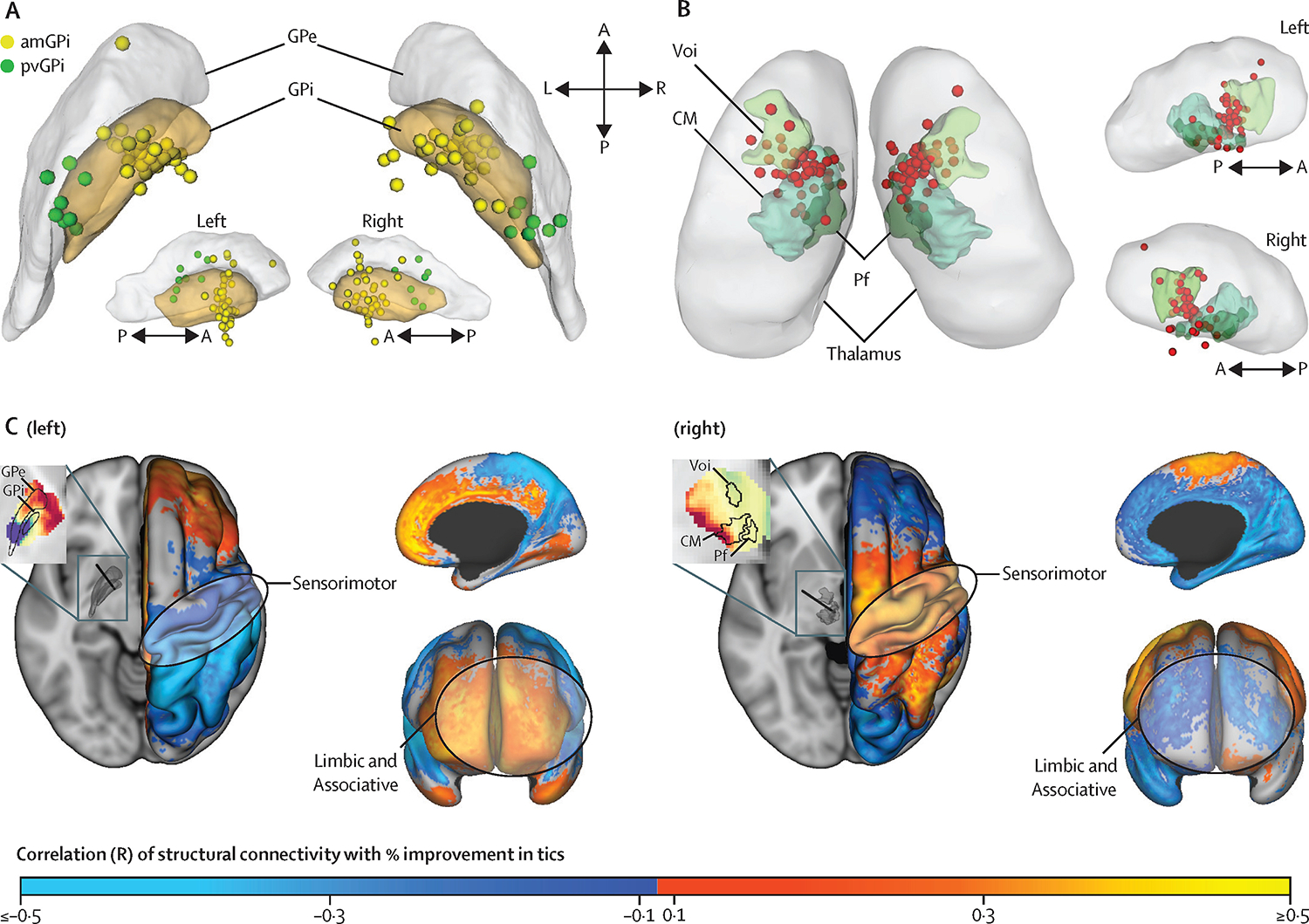
Adapted with permission from Johnson and colleagues.109,118 Active contact locations (represented by spheres) varied across patients with Tourette syndrome implanted with deep brain stimulation in (A) the pallidum (30 patients; yellow represents contacts targeted to amGPi and green pvGPi) and (B) the centromedian regions of the thalamus (33 patients; red contacts targeted to centromedian regions of the thalamus). (C) With pallidal deep brain stimulation (of either the amGPi or pvGPi), higher structural connectivity from the site of stimulation to limbic and associative networks was positively correlated with a reduction in tic severity (left). With thalamic deep brain stimulation, higher structural connectivity from the site of stimulation to sensorimotor networks was positively correlated with a reduction in tic severity (right). CM=centromedian nucleus. GPe=globus pallidus externus. GPi=globus pallidus internus. Pf=parafascicular nucleus. Voi=ventro-oralis internus.
Another promising area of research is the use of neurophysiology to guide deep brain stimulation. Closed-loop deep brain stimulation controlled by low-frequency thalamic activity, a potential marker that has been linked to tics in Tourette syndrome,69 has shown promising results. A case study reported a 48% improvement in tic severity as measured by the YGTSS and a 63% improvement in projected battery life compared with continuous stimulation.68 Further studies are needed to determine the long-term efficacy of closed-loop stimulation for Tourette syndrome treatment.
Conclusions and future directions
Research over the past 5 years has substantially contributed to our understanding of the clinical presentation, genetics, and pathophysiology of Tourette syndrome, which has enabled progress towards development of new therapies and improvement of existing therapies for tics and associated comorbidities. New insights into the typical time course and predictors of tics and comorbidities might improve the ability of clinicians to diagnose Tourette syndrome and to determine effective treatment plans. Multicentre consortia have transformed genetic research for Tourette syndrome and have identified gene variants potentially associated with increased risk, which could be relevant for diagnosis or developing novel therapeutic targets. Although experts generally agree that deficits in inhibition of behaviour underlie Tourette syndrome, new models propose that it might encompass over-learned behaviours or deficits in social behavioural brain networks. These models might help to explain both tics and the behavioural symptoms of Tourette syndrome and could lead to new targets for pharmacological or neuromodulation therapies. Behavioural therapies such as CBIT can be highly effective in improving tics, and access is continuing to expand with online and telehealth options. Finally, new predictors of response to deep brain stimulation and novel investigational tools are rapidly improving our understanding of the neurophysiology underlying Tourette syndrome, which might guide neurosurgical targeting and stimulation programming to improve the efficacy of deep brain stimulation therapy for treatment-refractory symptoms.
Despite progress in our understanding of Tourette syndrome, several unsolved challenges affect both research and clinical domains. To address these challenges, aggregating data across centres will be crucial, especially for research studies requiring large patient cohorts (eg, neuroimaging or genetics) and those with a small candidate population (eg, neuromodulation). Several research organisations and multicentre consortia have been established to pool data, resources, and multidisciplinary expertise across Tourette syndrome research domains.122 Examples of active consortia include the ESSTS,123 several international organisations focused on large genetics studies,124 and the International Tourette Syndrome Deep Brain Stimulation Registry and Database125 and the Neuroimaging Consortium,126 both of which are supported by the Tourette Association of America. Multicentre research initiatives and open access datasets will be essential to advance knowledge and to refine treatments.
Future research should aim to further our understanding of the pathophysiology of Tourette syndrome and translate this knowledge to refine therapies. Objective measures of tic severity are needed to track symptoms longitudinally and in naturalistic environments to better capture patient-specific fluctuations and supplement clinician-administered rating scales. Robust predictors of which patients' symptoms will improve over time and which patients will experience severe tics into adulthood will be crucial to establish timely and effective treatment plans. In particular, patients whose symptoms are likely to persevere into adulthood could be candidates to opt for behavioural and medication therapy and establish a longitudinal treatment plan earlier. To develop more effective treatments, we will need a clearer understanding of clinical subtypes of Tourette syndrome (ie, combinations of motor tics, phonic tics, and behavioural or psychiatric comorbidities of varying complexity and severity), which could be stratified using common symptoms across diagnoses, genetics, neuroimaging, or neurophysiological measures. Additionally, genetic data will need to be connected to neurobiological mechanisms through consortia, such as the Psychiatric Cell Map Initiative, to further uncover the protein complexes and functional pathways implicated in Tourette syndrome.127
Neuroimaging and neurophysiology in deep brain stimulation have the potential to provide objective markers to guide neurosurgical targeting and stimulation programming, which could presumably improve the efficacy of this invasive therapy for selected individuals with severe Tourette syndrome. Future studies should aim to further develop patient-specific approaches to optimise deep brain stimulation via interdisciplinary, multicentre collaborations and prioritise prospective validation of predictors to enable clinical translation. Finally, across all disciplines and research topics, patient organisations and advocacy groups will be integral to ensure that research priorities best serve the needs of individuals with Tourette syndrome.
Supplementary Material
Acknowledgments
We would like to thank Erica Rodriguez for the figure illustrations.
Footnotes
Declaration of interests
KAJ reports receiving fellowship funding from the National Science Foundation and travel grant awards from the International Congress of Parkinson's Disease and Movement Disorders. AG has received grant funding from the National Institutes of Health (NIH; R01NS096008) and the National Science Foundation (NSF PECASE 1553482); support from the Tourette Association of America; device donations from Medtronic under an NIH contract; and serves as a board member of the Brain Computer Interfaces Society. KDF reports receiving research support and fellowship support from Medtronic and Boston Scientific and research support from Functional Neuromodulation. CRB has received support from the NIH (UH3 NS119844) and has served as a consultant for NeuraModix. MSO serves as a medical advisor for the Parkinson's Foundation; has received research grants from NIH, Parkinson's Foundation, the Michael J Fox Foundation, the Parkinson Alliance, Smallwood Foundation, the Bachmann-Strauss Foundation, the Tourette Syndrome Association, and the UF Foundation; has received support for research by NIH (R01 NR014852, R01NS096008, UH3NS119844, and U01NS119562); and is principal investigator of the NIH R25NS108939 Training Grant. All other authors declare no competing interests.
Search strategy and selection criteria
We searched PubMed for articles published between Jan 1, 2016, and July 1, 2022, and checked reference lists in relevant articles. Search terms used were “Tourette syndrome”, or “tics”, in combination with “comorbidities”, “pathophysiology”, or “treatment” without language restrictions. We chose original research articles and select review papers on the basis of originality and relevance to this Review.
References
- 1.Gilles de la Tourette G. Étude sur une affection nerveuse caractérisée par de l'incoordination motrice accompagnée d'écholalie et de coprolalie. Arch Neurol, 9 (1885), pp. 19–42. [Google Scholar]
- 2.Scharf JM, Miller LL, Gauvin CA, Alabiso J, Mathews CA, Ben-Shlomo Y. Population prevalence of Tourette syndrome: a systematic review and meta-analysis. Mov Disord, 30 (2015), pp. 221–228. [DOI] [PubMed] [Google Scholar]
- 3.Levine JLS, Szejko N, Bloch MH. Meta-analysis: adulthood prevalence of Tourette syndrome. Prog Neuropsychopharmacol Biol Psychiatry, 95 (2019), Article 109675. [DOI] [PubMed] [Google Scholar]
- 4.Garcia-Delgar B, Servera M, Coffey BJ, et al. Tic disorders in children and adolescents: does the clinical presentation differ in males and females? A report by the EMTICS group. Eur Child Adolesc Psychiatry (2021). [DOI] [PubMed] [Google Scholar]
- 5.Sambrani T, Jakubovski E, Müller-Vahl KR. New insights into clinical characteristics of Gilles de la Tourette syndrome: findings in 1032 patients from a single German center. Front Neurosci, 10 (2016), p. 415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barnea M, Benaroya-Milshtein N, Gilboa-Sechtman E, et al. Subjective versus objective measures of tic severity in Tourette syndrome—the influence of environment. Psychiatry Res, 242 (2016), pp. 204–209. [DOI] [PubMed] [Google Scholar]
- 7.Robinson S, Hedderly T. Novel psychological formulation and treatment of “tic attacks” in Tourette syndrome. Front Pediatr, 4 (2016), p. 46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jankovic J. Tourette syndrome. Phenomenology and classification of tics. Neurol Clin, 15 (1997), pp. 267–275. [DOI] [PubMed] [Google Scholar]
- 9.Schubert L, Verrel J, Behm A, Bäumer T, Beste C, Münchau A. Inter-individual differences in urge-tic associations in Tourette syndrome. Cortex, 143 (2021), pp. 80–91. [DOI] [PubMed] [Google Scholar]
- 10.Conelea CA, Wellen B, Woods DW, et al. Patterns and predictors of tic suppressibility in youth with Tic disorders. Front Psychiatry, 9 (2018), p. 188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Baizabal-Carvallo JF, Alonso-Juarez M, Jankovic J. Self-injurious behavior in Tourette syndrome. J Neurol, 269 (2022), pp. 2453–2459. [DOI] [PubMed] [Google Scholar]
- 12.Stafford M, Cavanna AE. Prevalence and clinical correlates of self-injurious behavior in Tourette syndrome. Neurosci Biobehav Rev, 113 (2020), pp. 299–307. [DOI] [PubMed] [Google Scholar]
- 13.Claudio-Campos K, Stevens D, Koo SW, et al. Is persistent motor or vocal tic disorder a milder form of Tourette syndrome? Mov Disord, 36 (2021), pp. 1899–1910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Müller-Vahl KR, Sambrani T, Jakubovski E. Tic disorders revisited: introduction of the term “tic spectrum disorders”. Eur Child Adolesc Psychiatry, 28 (2019), pp. 1129–1135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Martino D, Pringsheim TM, Cavanna AE, et al. Systematic review of severity scales and screening instruments for tics: critique and recommendations. Mov Disord, 32 (2017), pp. 467–473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Szejko N, Robinson S, Hartmann A, et al. European clinical guidelines for Tourette syndrome and other tic disorders—version 2.0. Part I: assessment. Eur Child Adolesc Psychiatry, 31 (2022), pp. 383–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wand R, Shady G, Broder R, Furer P, Staley D. Tourette syndrome: issues in diagnosis. Neurosci Biobehav Rev, 16 (1992), pp. 449–451. [DOI] [PubMed] [Google Scholar]
- 18.Mol Debes NMM, Hjalgrim H, Skov L. Limited knowledge of Tourette syndrome causes delay in diagnosis. Neuropediatrics, 39 (2008), pp. 101–105. [DOI] [PubMed] [Google Scholar]
- 19.Openneer TJC, Huyser C, Martino D, Schrag A, Hoekstra PJ, Dietrich A. Clinical precursors of tics: an EMTICS study. J Child Psychol Psychiatry, 63 (2022), pp. 305–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hartmann A, Millet B. Repetitive movements and behaviors in neurological and psychiatric practice: distinctions and similarities between Tourette disorder and obsessive-compulsive disorder. Rev Neurol, 174 (2018), pp. 199–202. [DOI] [PubMed] [Google Scholar]
- 21.Szejko N, Müller-Vahl KR. Challenges in the diagnosis and assessment in patients with Tourette syndrome and comorbid obsessive-compulsive disorder. Neuropsychiatr Dis Treat, 17 (2021), pp. 1253–1266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ganos C, Martino D, Espay AJ, Lang AE, Bhatia KP, Edwards MJ. Tics and functional tic-like movements: can we tell them apart? Neurology, 93 (2019), pp. 750–758. [DOI] [PubMed] [Google Scholar]
- 23.Paulus T, Bäumer T, Verrel J, et al. Pandemic tic-like behaviors following social media consumption. Mov Disord (2021). published online Sept 24. 10.1002/mds.28800 [DOI] [PubMed] [Google Scholar]
- 24.Pringsheim T, Ganos C, McGuire JF, et al. Rapid onset functional tic-like behaviors in young females during the COVID-19 pandemic. Mov Disord, 36 (2021), pp. 2707–2713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Leckman JF, Zhang H, Vitale A, et al. Course of tic severity in Tourette syndrome: the first two decades. Pediatrics, 102 (1998), pp. 14–19. [DOI] [PubMed] [Google Scholar]
- 26.Black KJ, Kim S, Yang NY, Greene DJ. Course of tic disorders over the lifespan. Curr Dev Disord Rep, 8 (2021), pp. 121–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Groth C, Mol Debes N, Rask CU, Lange T, Skov L. Course of Tourette Syndrome and comorbidities in a large prospective clinical study. J Am Acad Child Adolesc Psychiatry, 56 (2017), pp. 304–312. [DOI] [PubMed] [Google Scholar]
- 28.Groth C, Skov L, Lange T, Debes NM. Predictors of the clinical course of Tourette syndrome: a longitudinal study. J Child Neurol, 34 (2019), pp. 913–921. [DOI] [PubMed] [Google Scholar]
- 29.Lin H, Katsovich L, Ghebremichael M, et al. Psychosocial stress predicts future symptom severities in children and adolescents with Tourette syndrome and/or obsessive-compulsive disorder. J Child Psychol Psychiatry, 48 (2007), pp. 157–166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hirschtritt ME, Lee PC, Pauls DL, et al. Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry, 72 (2015), pp. 325–333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Meier SM, Dalsgaard S, Mortensen PB, Leckman JF, Plessen KJ. Mortality risk in a nationwide cohort of individuals with tic disorders and with tourette syndrome. Mov Disord, 32 (2017), pp. 605–609. [DOI] [PubMed] [Google Scholar]
- 32.Huisman-van Dijk HM, Matthijssen SJMA, Stockmann RTS, Fritz AV, Cath DC. Effects of comorbidity on Tourette's tic severity and quality of life. Acta Neurol Scand, 140 (2019), pp. 390–398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mataix-Cols D, Isomura K, Pérez-Vigil A, et al. Familial risks of Tourette syndrome and chronic tic disorders. A population-based cohort study. JAMA Psychiatry, 72 (2015), pp. 787–793. [DOI] [PubMed] [Google Scholar]
- 34.Yu D, Sul JH, Tsetsos F, et al. Interrogating the genetic determinants of Tourette's syndrome and other tic disorders through genome-wide association studies. Am J Psychiatry, 176 (2019), pp. 217–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Abdulkadir M, Mathews CA, Scharf JM, et al. Polygenic risk scores derived from a Tourette syndrome genome-wide association study predict presence of tics in the avon longitudinal study of parents and children cohort. Biol Psychiatry, 85 (2019), pp. 298–304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Leivonen S, Scharf JM, Mathews CA, et al. Parental Psychopathology and Tourette syndrome/chronic tic disorder in offspring: a nationwide case-control study. J Am Acad Child Adolesc Psychiatry, 56 (2017), pp. 297–303.e4. [DOI] [PubMed] [Google Scholar]
- 37.Anttila V, Bulik-Sullivan B, Finucane HK, et al. Analysis of shared heritability in common disorders of the brain. Science, 360 (2018), Article eaap8757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Yang Z, Wu H, Lee PH, et al. investigating shared genetic basis across Tourette Syndrome and comorbid neurodevelopmental disorders along the impulsivity-compulsivity spectrum. Biol Psychiatry, 90 (2021), pp. 317–327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Willsey AJ, Fernandez TV, Yu D, et al. De novo coding variants are strongly associated with Tourette disorder. Neuron, 94 (2017), pp. 486–499.e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cappi C, Oliphant ME, Péter Z, et al. De novo damaging DNA coding mutations are associated with obsessive-compulsive disorder and overlap with Tourette's disorder and autism. Biol Psychiatry, 87 (2020), pp. 1035–1044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Depienne C, Ciura S, Trouillard O, et al. Association of rare genetic variants in opioid receptors with Tourette syndrome. Tremor Other Hyperkinet Mov, 9 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ercan-Sencicek AG, Stillman AA, Ghosh AK, et al. L-histidine decarboxylase and Tourette's syndrome. N Engl J Med, 362 (2010), pp. 1901–1908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Wang S, Mandell JD, Kumar Y, et al. De novo sequence and copy number variants are strongly associated with Tourette disorder and implicate cell polarity in pathogenesis. Cell Rep, 24 (2018), p. 3441–3454.e12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Tsetsos F, Yu D, Sul JH, et al. Synaptic processes and immune-related pathways implicated in Tourette syndrome. Transl Psychiatry, 11 (2021), p. 56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Cao X, Zhang Y, Abdulkadir M, et al. Whole-exome sequencing identifies genes associated with Tourette's disorder in multiplex families. Mol Psychiatry, 26 (2021), pp. 6937–6951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Jones HF, Han VX, Patel S, et al. Maternal autoimmunity and inflammation are associated with childhood tics and obsessive-compulsive disorder: transcriptomic data show common enriched innate immune pathways. Brain Behav Immun, 94 (2021), pp. 308–317. [DOI] [PubMed] [Google Scholar]
- 47.Han VX, Patel S, Jones HF, Dale RC. Maternal immune activation and neuroinflammation in human neurodevelopmental disorders. Nat Rev Neurol, 17 (2021), pp. 564–579. [DOI] [PubMed] [Google Scholar]
- 48.Sarchioto M, Howe F, Dumitriu IE, et al. Analyses of peripheral blood dendritic cells and magnetic resonance spectroscopy support dysfunctional neuro-immune crosstalk in Tourette syndrome. Eur J Neurol, 28 (2021), pp. 1910–1921. [DOI] [PubMed] [Google Scholar]
- 49.Nielsen AN, Gratton C, Church JA, et al. Atypical functional connectivity in Tourette syndrome differs between children and adults. Biol Psychiatry, 87 (2020), pp. 164–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Marín O. Developmental timing and critical windows for the treatment of psychiatric disorders. Nat Med, 22 (2016), pp. 1229–1238. [DOI] [PubMed] [Google Scholar]
- 51.Martino D, Ganos C, Worbe Y. Neuroimaging applications in Tourette's syndrome. Int Rev Neurobiol, 143 (2018), pp. 65–108. [DOI] [PubMed] [Google Scholar]
- 52.Worbe Y, Marrakchi-Kacem L, Lecomte, et al. Altered structural connectivity of cortico-striato-pallido-thalamic networks in Gilles de la Tourette syndrome. Brain, 138 (2015), pp. 472–482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Mink JW. Basal ganglia dysfunction in Tourette's syndrome: a new hypothesis. Pediatr Neurol, 25 (2001), pp. 190–198. [DOI] [PubMed] [Google Scholar]
- 54.Kalanithi PSA, Zheng W, Kataoka Y, et al. Altered parvalbumin-positive neuron distribution in basal ganglia of individuals with Tourette syndrome. Proc Natl Acad Sci USA, 102 (2005), pp. 13307–13312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Kataoka Y, Kalanithi PSA, Grantz H, et al. Decreased number of parvalbumin and cholinergic interneurons in the striatum of individuals with Tourette syndrome. J Comp Neurol, 518 (2010), pp. 277–291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Tremblay L, Worbe Y, Thobois S, Sgambato-Faure V, Féger J. Selective dysfunction of basal ganglia subterritories: from movement to behavioral disorders. Mov Disord, 30 (2015), pp. 1155–1170. [DOI] [PubMed] [Google Scholar]
- 57.Rawji V, Modi S, Latorre A, et al. Impaired automatic but intact volitional inhibition in primary tic disorders. Brain, 143 (2020), pp. 906–919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Atkinson-Clement C, Porte C, de Liege A, et al. Impulsive prepotent actions and tics in Tourette disorder underpinned by a common neural network. Mol Psychiatry, 26 (2021), pp. 3548–3557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Morand-Beaulieu S, Grot S, Lavoie, Leclerc, Luck, Lavoie ME. The puzzling question of inhibitory control in Tourette syndrome: A meta-analysis. Neurosci Biobehav Rev, 80 (2017), pp. 240–262. [DOI] [PubMed] [Google Scholar]
- 60.Jackson GM, Draper A, Dyke K, Pépés SE, Jackson SR. Inhibition, disinhibition, and the control of action in Tourette syndrome. Trends Cogn Sci, 19 (2015), pp. 655–665. [DOI] [PubMed] [Google Scholar]
- 61.Maia TV, Conceição VA. Dopaminergic disturbances in Tourette syndrome: an integrative account. Biol Psychiatry, 84 (2018), pp. 332–344. [DOI] [PubMed] [Google Scholar]
- 62.Palminteri S, Pessiglione M. Reinforcement learning and Tourette Syndrome. Int Rev Neurobiol, 112 (2013), pp. 131–153. [DOI] [PubMed] [Google Scholar]
- 63.Delorme C, Salvador A, Valabrègue R, et al. Enhanced habit formation in Gilles de la Tourette syndrome. Brain, 139 (2016), pp. 605–615. [DOI] [PubMed] [Google Scholar]
- 64.Conceição VA, Dias Â, Farinha AC, Maia TV. Premonitory urges and tics in Tourette syndrome: computational mechanisms and neural correlates. Curr Opin Neurobiol, 46 (2017), pp. 187–199. [DOI] [PubMed] [Google Scholar]
- 65.Jackson SR, Loayza J, Crighton M, Sigurdsson HP, Dyke K, Jackson GM. The role of the insula in the generation of motor tics and the experience of the premonitory urge-to-tic in Tourette syndrome. Cortex, 126 (2020), pp. 119–133. [DOI] [PubMed] [Google Scholar]
- 66.Marceglia S, Servello D, Foffani, et al. Thalamic single-unit and local field potential activity in Tourette syndrome. Mov Disord, 25 (2010), pp. 300–308. [DOI] [PubMed] [Google Scholar]
- 67.Neumann W-J, Huebl J, Brücke C, et al. Pallidal and thalamic neural oscillatory patterns in Tourette's syndrome. Ann Neurol, 84 (2018), pp. 505–514. [DOI] [PubMed] [Google Scholar]
- 68.Molina R, Okun MS, Shute JB, et al. Report of a patient undergoing chronic responsive deep brain stimulation for Tourette syndrome: proof of concept. J Neurosurg, 129 (2018), pp. 308–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Cagle JN, Okun MS, Opri E, et al. Differentiating tic electrophysiology from voluntary movement in the human thalamocortical circuit. J Neurol Neurosurg Psychiatry, 91 (2020), pp. 533–539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Shute JB, Okun MS, Opri E, et al. Thalamocortical network activity enables chronic tic detection in humans with Tourette syndrome. Neuroimage Clin, 12 (2016), pp. 165–172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Zauber SE, Ahn S, Worth RM, Rubchinsky LL. Oscillatory neural activity of anteromedial globus pallidus internus in Tourette syndrome. Clin Neurophysiol, 125 (2014), pp. 1923–1924. [DOI] [PubMed] [Google Scholar]
- 72.Jimenez-Shahed J, Telkes I, Viswanathan A, Ince NF. GPi oscillatory activity differentiates tics from the resting state, voluntary movements, and the unmedicated Parkinsonian state. Front Neurosci, 10 (2016), p. 436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Zhu GY, Geng XY, Zhang RL, et al. Deep brain stimulation modulates pallidal and subthalamic neural oscillations in Tourette's syndrome. Brain Behav, 9 (2019), Article e01450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Wilken M, Cerquetti D, Rossi M, Obeso JA, Merello M. Low-frequency oscillations at the limbic globus pallidus internus seem to be associated with premonitory urges in Tourette's syndrome Mov Disord, 36 (2021), pp. 2966–2967. [DOI] [PubMed] [Google Scholar]
- 75.Albin RL. Tourette syndrome: a disorder of the social decision-making network. Brain, 141 (2018), pp. 332–347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Rae CL, Polyanska L, Gould van Praag CD, et al. Face perception enhances insula and motor network reactivity in Tourette syndrome. Brain, 141 (2018), pp. 3249–3261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Kleimaker M, Takacs A, Conte, et al. Increased perception-action binding in Tourette syndrome. Brain, 143 (2020), pp. 1934–1945. [DOI] [PubMed] [Google Scholar]
- 78.Pringsheim T, Okun MS, Müller-Vahl K, et al. Practice guideline recommendations summary: treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology, 92 (2019), pp. 896–906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Pringsheim T, Holler-Managan Y, Okun MS, et al. Comprehensive systematic review summary: treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology, 92 (2019), pp. 907–915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Andrén P, Jakubovski E, Murphy TL, et al. European clinical guidelines for Tourette syndrome and other tic disorders—version 2.0. Part II: psychological interventions. Eur Child Adolesc Psychiatry, 31 (2021), pp. 403–423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Roessner V, Eichele H, Stern JS, et al. European clinical guidelines for Tourette syndrome and other tic disorders—version 2.0. Part III: pharmacological treatment. Eur Child Adolesc Psychiatry, 31 (2022), pp. 425–441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Rizzo R, Pellico A, Silvestri PR, Chiarotti F, Cardona F. A randomized controlled trial comparing behavioral, educational, and pharmacological treatments in youths with chronic tic disorder or Tourette Syndrome. Front Psychiatry, 9 (2018), p. 100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Piacentini J, Woods DW, Scahill L, et al. Behavior therapy for children with Tourette disorder: a randomized controlled trial. JAMA, 303 (2010), pp. 1929–1937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Wilhelm S, Deckersbach T, Coffey BJ, Bohne A, Peterson AL, Baer L. Habit reversal versus supportive psychotherapy for Tourette's disorder: a randomized controlled trial. Am J Psychiatry, 160 (2003), pp. 1175–1177. [DOI] [PubMed] [Google Scholar]
- 85.Verdellen CW, Keijsers GP, Cath DC, Hoogduin CA. Exposure with response prevention versus habit reversal in Tourettes's syndrome: a controlled study. Behav Res Ther, 42 (2004), pp. 501–511. [DOI] [PubMed] [Google Scholar]
- 86.Nissen JB, Kaergaard M, Laursen L, Parner E, Thomsen PH. Combined habit reversal training and exposure response prevention in a group setting compared to individual training: a randomized controlled clinical trial. Eur Child Adolesc Psychiatry, 28 (2019), pp. 57–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Heijerman-Holtgrefe AP, Verdellen CWJ, van de Griendt JMTM, et al. Tackle your tics: pilot findings of a brief, intensive group-based exposure therapy program for children with tic disorders. Eur Child Adolesc Psychiatry, 30 (2021), pp. 461–473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Ricketts EJ, Goetz AR, Capriotti MR, et al. A randomized waitlist-controlled pilot trial of voice over internet protocol-delivered behavior therapy for youth with chronic tic disorders. J Telemed Telecare, 22 (2016), pp. 153–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Andrén P, Aspvall K, Fernández de la Cruz L, et al. Therapist-guided and parent-guided internet-delivered behaviour therapy for paediatric Tourette's disorder: a pilot randomised controlled trial with long-term follow-up. BMJ Open, 9 (2019), Article e024685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Sukhodolsky DG, Woods DW, Piacentini J, et al. Moderators and predictors of response to behavior therapy for tics in Tourette syndrome. Neurology, 88 (2017), pp. 1029–1036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Gilbert DL, Murphy TK, Jankovic J, et al. Ecopipam, a D1 receptor antagonist, for treatment of Tourette syndrome in children: a randomized, placebo-controlled crossover study. Mov Disord, 33 (2018), pp. 1272–1280. [DOI] [PubMed] [Google Scholar]
- 92.Farber RH, Angelov A, Kim K, Carmack T, Thai-Cuarto D, Roberts E. Clinical development of valbenazine for tics associated with Tourette syndrome. Expert Rev Neurother, 21 (2021), pp. 393–404. [DOI] [PubMed] [Google Scholar]
- 93.Jankovic J, Jimenez-Shahed J, Budman C, et al. Deutetrabenazine in tics associated with tourette syndrome. Tremor Other Hyperkinet Mov, 6 (2016), p. 422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Jankovic J, Coffey B, Claassen D, et al. Safety and efficacy of flexible-dose deutetrabenazine in children and adolescents with tourette syndrome. JAMA Netw Open, 4 (2021), Article e2128204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Milosev LM, Psathakis N, Szejko N, Jakubovski E, Müller-Vahl KR. Treatment of Gilles de la Tourette syndrome with cannabis-based medicine: results from a retrospective analysis and online survey. Cannabis Cannabinoid Res, 4 (2019), pp. 265–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Thaler A, Arad S, Schleider LB-L, et al. Single center experience with medical cannabis in Gilles de la Tourette syndrome. Parkinsonism Relat Disord, 61 (2019), pp. 211–213. [DOI] [PubMed] [Google Scholar]
- 97.Black N, Stockings E, Campbell G, et al. Cannabinoids for the treatment of mental disorders and symptoms of mental disorders: a systematic review and meta-analysis. Lancet Psychiatry, 6 (2019), pp. 995–1010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Khan R, Naveed S, Mian N, Fida A, Raafey MA, Aedma KK. The therapeutic role of cannabidiol in mental health: a systematic review. J Cannabis Res, 2 (2020), p. 2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Tibbo PG, McKee KA, Meyer JH, et al. Are there therapeutic benefits of cannabinoid products in adult mental illness? Can J Psychiatry, 66 (2021), pp. 185–194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Jakubovski E, Pisarenko A, Fremer C, et al. The CANNA-TICS study protocol: a randomized multi-center double-blind placebo controlled trial to demonstrate the efficacy and safety of nabiximols in the treatment of adults with chronic tic disorders. Front Psychiatry, 11 (2020), Article 575826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Dyke K, Jackson GM, Nixon E, Jackson SR. Effects of single-session cathodal transcranial direct current stimulation on tic symptoms in Tourette's syndrome. Exp Brain Res, 237 (2019), pp. 2853–2863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Grados M, Huselid R, Duque-Serrano L. Transcranial magnetic stimulation in Tourette syndrome: a historical perspective, its current use and the influence of comorbidities in treatment response. Brain Sci, 8 (2018), p. E129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Landeros-Weisenberger A, Mantovani A, Motlagh MG, et al. Randomized sham controlled double-blind trial of repetitive transcranial magnetic stimulation for adults with severe Tourette syndrome. Brain Stimul, 8 (2015), pp. 574–581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Morera Maiquez B, Sigurdsson HP, Dyke K, et al. Entraining movement-related brain oscillations to suppress tics in Tourette syndrome. Curr Biol, 30 (2020), pp. 2334–2342.e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Sukhodolsky DG, Walsh C, Koller WN, et al. Randomized, sham-controlled trial of real-time functional magnetic resonance imaging neurofeedback for tics in adolescents with Tourette syndrome. Biol Psychiatry, 87 (2020), pp. 1063–1070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Martino D, Deeb W, Jimenez-Shahed J, et al. The 5 pillars in Tourette syndrome deep brain stimulation patient selection: present and future. Neurology, 96 (2021), pp. 664–676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Martinez-Ramirez D, Jimenez-Shahed J, Leckman JF, et al. Efficacy and safety of deep brain stimulation in Tourette syndrome: the international Tourette syndrome deep brain stimulation public database and registry. JAMA Neurol, 75 (2018), pp. 353–359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Baldermann JC, Schüller T, Huys D, et al. Deep brain stimulation for Tourette-syndrome: a systematic review and meta-analysis. Brain Stimul, 9 (2016), pp. 296–304. [DOI] [PubMed] [Google Scholar]
- 109.Johnson KA, Fletcher PT, Servello D, et al. Image-based analysis and long-term clinical outcomes of deep brain stimulation for Tourette syndrome: a multisite study. J Neurol Neurosurg Psychiatry, 90 (2019), pp. 1078–1090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Mahajan UV, Purger DA, Mantovani A, et al. Deep brain stimulation results in greater symptomatic improvement in Tourette syndrome than conservative measures: a meta-analysis. Stereotact Funct Neurosurg, 98 (2020), pp. 270–277. [DOI] [PubMed] [Google Scholar]
- 111.Kefalopoulou Z, Zrinzo L, Jahanshahi M, et al. Bilateral globus pallidus stimulation for severe Tourette's syndrome: a double-blind, randomised crossover trial. Lancet Neurol, 14 (2015), pp. 595–605. [DOI] [PubMed] [Google Scholar]
- 112.Welter M-L, Houeto J-L, Thobois S, et al. Anterior pallidal deep brain stimulation for Tourette's syndrome: a randomised, double-blind, controlled trial. Lancet Neurol, 16 (2017), pp. 610–619. [DOI] [PubMed] [Google Scholar]
- 113.Baldermann JC, Kuhn J, Schüller T, et al. Thalamic deep brain stimulation for Tourette syndrome: a naturalistic trial with brief randomized, double-blinded sham-controlled periods. Brain Stimul, 14 (2021), pp. 1059–1067. [DOI] [PubMed] [Google Scholar]
- 114.Müller-Vahl KR, Szejko N, Saryyeva, et al. Randomized double-blind sham-controlled trial of thalamic versus GPi stimulation in patients with severe medically refractory Gilles de la Tourette syndrome. Brain Stimul, 14 (2021), pp. 662–675. [DOI] [PubMed] [Google Scholar]
- 115.Wehmeyer L, Schüller T, Kiess J, et al. Target-specific effects of deep brain stimulation for Tourette syndrome: a systematic review and meta-analysis. Front Neurol, 12 (2021), Article 769275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Servello D, Galbiati TF, Balestrino R, et al. Deep brain stimulation for Gilles de la Tourette syndrome: toward limbic targets. Brain Sci, 10 (2020), p. 301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Andrade P, Heiden P, Hoevels M, et al. Modulation of fibers to motor cortex during thalamic DBS in Tourette patients correlates with tic reduction. Brain Sci, 10 (2020), p. 302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Johnson KA, Duffley G, Anderson DN, et al. Structural connectivity predicts clinical outcomes of deep brain stimulation for Tourette syndrome. Brain, 143 (2020), pp. 2607–2623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Morishita T, Sakai Y, Iida H, et al. Neuroanatomical considerations for optimizing thalamic deep brain stimulation in Tourette syndrome. J Neurosurg, 136 (2021), pp. 231–241. [DOI] [PubMed] [Google Scholar]
- 120.Jo HJ, McCairn KW, Gibson WS, et al. Global network modulation during thalamic stimulation for Tourette syndrome. Neuroimage Clin, 18 (2018), pp. 502–509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Johnson KA, Duffley G, Foltynie T, et al. Basal ganglia pathways associated with therapeutic pallidal deep brain stimulation for Tourette syndrome. Biol Psychiatry Cogn Neurosci Neuroimaging, 6 (2021), pp. 961–972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Kleimaker A, Kleimaker M, Behm A, et al. Networks in the field of Tourette syndrome. Front Neurol, 12 (2021), Article 624858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Rickards H, Paschou P, Rizzo R, Stern JS. A brief history of the European Society for the Study of Tourette syndrome. Behav Neurol, 27 (2013), pp. 3–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Georgitsi M, Willsey AJ, Mathews CA, State M, Scharf JM, Paschou P. The genetic etiology of Tourette syndrome: large-scale collaborative efforts on the precipice of discovery. Front Neurosci, 10 (2016), p. 351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Deeb W, Rossi PJ, Porta M, et al. The international deep brain stimulation registry and database for Gilles de la Tourette syndrome: how does it work? Front Neurosci, 10 (2016), p. 170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Greene DJ, Williams Iii AC, Koller JM, Schlaggar BL, Black KJ. Brain structure in pediatric Tourette syndrome. Mol Psychiatry, 22 (2017), pp. 972–980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Willsey AJ, Morris MT, Wang, et al. The psychiatric cell map initiative: a convergent systems biological approach to illuminating key molecular pathways in neuropsychiatric disorders. Cell, 174 (2018), pp. 505–520. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.